Throughout history man has tried to straighten out that which nature has bent, twisted, or curved. Hippocrates not only gave a name to scoliosis but he also tried to correct it. Over the centuries since then physicians have used a wide, and sometimes strange, variety of devices to straighten a crooked spine.
In today’s world when a growing adolescent is diagnosed with progressive idiopathic scoliosis and the curve is between 25 and 40 degrees, the physician will prescribe the wearing of a brace to keep the curve from worsening. Depending on the severity of the curve, the curve pattern, and the amount of growth remaining, the physician may not wait to document progression but will prescribe bracing on the initial visit.
In 1985, the Scoliosis Research Society (SRS) initiated a study to investigate the effectiveness of bracing as a treatment for scoliosis. Many previous studies of full time bracing showed that braces stop about 80% of curves. All of these studies, however, were “uncontrolled” which means there were no simultaneous groups of untreated, unbraced patients for comparison. Therefore, there was some doubt that brace treatment of scoliosis was effective, and concern that bracing may be no different than “natural history” or what happens when no treatment is undertaken. In the SRS controlled clinical trial, involving centers from around the world and conducted by Dr. Alf L. Nachemson Sahlgren Hospital, Gothenberg Sweden, patients of the same age, curve pattern and curve severity were divided into two groups, one treated with bracing, one not treated. As reported in the 1993 issue of the Spinal Connection, results of this study demonstrated with statistical certainty that bracing is effective compared to natural history.
In another study by Drs. John Lonstein and Robert Winter, the records and X-rays of 1,020 patients treated with the Milwaukee Brace were reviewed and compared with the findings of a study by Drs. Lonstein and J.M. Carlson which documented patients at the same hospitals who had not been braced but who had been followed for progression of the curve. This retrospective study also showed that bracing is an effective treatment, halting the progression of the curve in statistically significant numbers compared with those patients not treated.
While it is true that there are some patients (20-25%) for whom bracing does not work and unfortunately, it is not possible to predict who they will be parents and physicians can be reassured by these recent findings that bracing for those youngsters who meet the generally accepted criteria is a wise course of action.
What does bracing achieve?
It is important for parents and patients to realize that the purpose of bracing is to keep the curve from progressing as a child grows. While the curve will demonstrate improvement during the time the child is braced, it will typically revert to its original degree of severity when the use of the brace is eventually discontinued at the cessation of growth. Some individuals do achieve permanent correction, but holding the curve to an acceptable level, thus avoiding surgery, should be deemed a success.
What Kinds of Braces are Used?
The Milwaukee Brace
The Milwaukee Brace was the first modern brace designed for the treatment of scoliosis. Developed by Drs. Walter Blount and Albert Schmidt of the Medical College of Wisconsin and Milwaukee’s Children’s Hospital in 1945, it underwent design changes over the years, reaching its present form around 1975. It is still used today, particularly for high thoracic curves. Metal bars in the front and back of the brace extend the length of the torso and are attached to a form-fitting plastic pelvic girdle and to a throat mold or ring which encircles the neck. Straps attached to the metal bars hold pressure pads, which are precisely placed depending on the individual’s curve pattern. While the bars hold the body erect, the neck ring keeps the head centered over the pelvis and the pads push against the curve. Everything works together to keep the body straight and to prevent progression of the curve while the patient is growing.
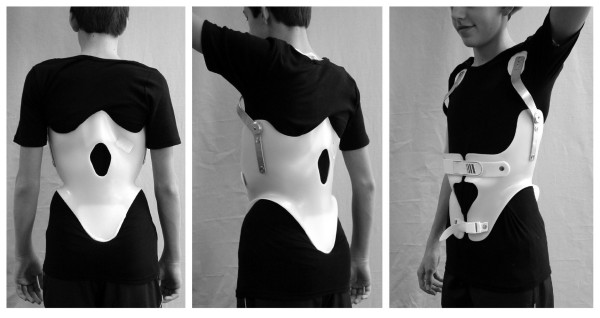
TLSO Braces
There are many TLSO (thoracic-lumbar-sacral orthosis) systems available today. They are also often referred to as “underarm” or “low profile” braces. They are made of modern plastic materials and are contoured to conform to the patient’s body. While they all differ somewhat in construction, they work on basically the same principle.
The Boston Brace
In the early seventies, the most popular of the TLSO systems, the Boston Brace, was developed by Dr. John Hall and Dr. William Miller of The Boston Children’s Hospital. The Boston Brace was the first brace to utilize symmetrical standardized modules eliminating the need for casting. It was alsothe brace used in the Scoliosis Research Society’s bracing study. The Boston Brace extends from below the breast to the beginning of the pelvic area in front and just below the scapulae to the middle of the buttocks in the back. It is designed to keep the lumbar area of the body in a flexed position by pushing the abdomen in and flattening the posterior lumbar contour. Pads are strategically placed to provide pressure to the curve, and areas of “relief” or “voids” are provided opposite the areas of pressure.
The Charleston Bending Brace
The Charleston Bending Brace was introduced in 1979. Developed by Dr. Frederick Reed and Mr. Ralph Hooper, CPO, this brace is worn only at night during sleep. It is molded to conform to the patient’s body while bending towards the convexity of the curve, thus “over-correcting” the curve during the eight hours it is worn. A preliminary study and subsequent longer term follow-up of those using the nighttime bending brace are encouraging, particularly for a single curve. Although the studies show no evidence of improved compliance the potential for a patient to wear a part-time brace, especially while sleeping, rather than the usual full-time (22-23 hours) regimen is cited as an important benefit.
“The purpose of bracing is to keep the curve from progressing as a child grows.”
To achieve a successful outcome from bracing it is necessary that a highly skilled orthotist or brace maker work hand in hand with the orthopedist to craft a brace precisely tailored to the patient’s needs. In many cases an exercise pro- gram is also provided. After that, the physician will have the patient return for routine checkups and order X-rays to make sure the brace is doing its job. He will prescribe periodic adjustments as necessary.
The brace is worn until the physician has determined that skeletal maturity has been reached at which time the patient will be gradually weaned from the brace.
Compliance on the patient’s part in wearing the brace according to the prescribed schedule is a crucial factor, of course. Several studies have demonstrated the importance that the mother’s attitude has on the child’s perception of her own condition and acceptance of treatment. While no one would suggest that adapting physically and psychologically to bracing is easy for children and teenagers, many studies show that after an initial adjustment period, youngsters who are braced live very normal lives, engaging in appropriate activities, including sports, and that they have good psychosocial adjustment, no matter which brace they wear.









{kind=link}
{kind=link}
{kind=link}
{kind=link}